
In this article
Open enrollment in 2023 plans has ended in most states
In the individual / family health insurance market (ie, coverage that people buy for themselves, as opposed to getting from an employer), open enrollment ended on January 15 in most states.
There are some state-run exchanges with different deadlines, although most of them are after January 15. Only Idaho opted to keep its open enrollment deadline in December.
As described below, Medicaid and CHIP enrollment are available year-round for eligible applicants, and Native Americans can also enroll year-round. And enrollment is available nationwide when people experience certain qualifying events. But there are also some states where other types of coverage can be obtained outside of open enrollment:
- Basic Health Programs in New York and Minnesota.
- The ConnectorCare program in Massachusetts (for people who are newly eligible or who haven’t enrolled before).
- The Covered Connecticut program allows eligible applicants to enroll anytime.
Depending on your circumstances, your opportunities to enroll after the end of the annual open enrollment period may be limited. But you may find that you can still get coverage without having to wait for the next annual open enrollment period.
A qualifying event at any time of the year will likely allow you to enroll
Applicants who experience a qualifying event gain access to a special enrollment period (SEP) to shop for plans in the exchange (or off-exchange, in most cases) with premium subsidies available in the exchange for eligible enrollees.
If you experience a qualifying event, be prepared to provide proof of it when you enroll. And in most cases, the current rules limit SEP plan changes to plans at the same metal level the person already has.
The state-run exchanges (ie, the ones that don’t use HealthCare.gov) can use their own discretion on this, but in general, if you’re enrolling mid-year, be prepared to provide proof of the qualifying event that triggered your special enrollment period, and know that you might not be able to switch to a more robust or less robust plan (eg, from bronze to gold or vice versa) during your SEP. And understand that in most — but not all — cases, the current SEP rules allow you to change your coverage but not necessarily go from being uninsured to insured. So you may be asked to provide proof of your prior coverage in addition to proof of the qualifying event.
For example, a permanent move to an area where different health plans are available will only trigger a SEP if you had coverage before the move. The same is true of getting married: In most cases, at least one spouse must have already had coverage in order for the marriage to trigger a SEP.
And without a qualifying event, major medical health insurance is not available outside of general open enrollment, on or off-exchange. This is very different from the pre-2014 individual health insurance market, where people could apply for coverage at any time. But of course, approval used to be contingent on health status, which is no longer the case.
Review the list of qualifying events that make you eligible for special enrollment.
Native Americans, those eligible for Medicaid/CHIP can enroll year-round
Native Americans can enroll in exchange plans year-round. There is also a year-round enrollment opportunity for subsidy-eligible applicants whose household income doesn’t exceed 150% of the poverty level.
And people who qualify for Medicaid or CHIP can also enroll at any time. Income limits are fairly high for CHIP eligibility, so be sure you check your state’s eligibility limits before assuming that your kids wouldn’t be eligible – benefits very much extend to middle-class households.
And in states where Medicaid has been expanded, a single individual earning up to $20,120 in 2023 can enroll in Medicaid once the 2023 federal poverty level guidelines are in effect (the limit is higher in Alaska and Hawaii). Most states have expanded Medicaid, but there are still 11 states where there is a Medicaid coverage gap and assistance is not available for most adults with income below the poverty level. (Note that South Dakota will expand Medicaid in July 2023, eliminating the coverage gap in that state at that point.)
Similarly, if you’re on Medicaid and your income increases to a level that makes you ineligible for Medicaid, you’ll have an opportunity to switch to a private plan at that point, with the loss of your Medicaid plan serving as the qualifying event that triggers a special enrollment period. (Through the end of March 2023, states are not disenrolling people from Medicaid even if they no longer meet the eligibility guidelines, but that will change starting in April 2023.)
The closest thing to ‘real’ insurance if you missed open enrollment
For people who didn’t enroll in coverage during open enrollment or the COVID-related enrollment window, aren’t eligible for employer-sponsored coverage or Medicaid/CHIP, and aren’t expecting a qualifying event later in the year, the options for 2023 coverage are limited to policies that are not regulated by the ACA and are thus not considered minimum essential coverage.
And most of these plans are designed to be supplemental coverage, rather than a person’s only health coverage. This includes things like limited-benefit plans, accident supplements, critical/specific-illness policies, dental/vision plans, and medical discount plans.
But there are a few types of coverage that are available year-round (generally only to fairly healthy individuals), and that can serve as stand-alone coverage in a pinch:
Farm Bureau plans in a few states
In Kansas, Tennessee, Indiana, Iowa, South Dakota, and Texas, members of Farm Bureau who are healthy enough to get through medical underwriting can enroll in Farm Bureau plans that are technically not considered insurance — and thus don’t have to comply with insurance regulations — but that are available for purchase year-round.
Health care sharing ministry plans
There are also health care sharing ministry plans available nearly everywhere, and although they are not compliant with insurance laws, they are better than nothing and are available year-round to people who meet their eligibility criteria.
Some people choose to combine a health care sharing ministry plan with a direct primary care membership, although this is still not an ideal arrangement — direct primary care plans still need to be combined with real major medical coverage in order to offer a truly comprehensive coverage safety net.
Short-term health plans
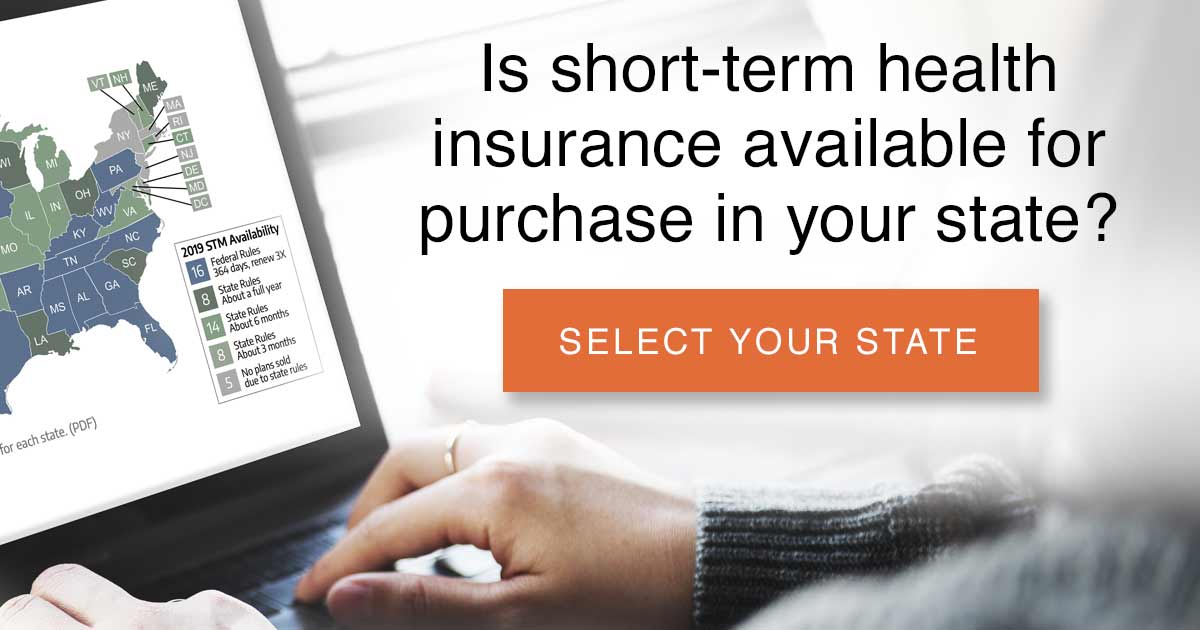 Short-term health insurance is available in most states (DC and 11 states do not have short-term plans available). It can serve as decent coverage if your other alternative is to remain uninsured. In most states, it’s the closest thing you can get to “real” health insurance if you find yourself needing to purchase a policy outside of open enrollment without a qualifying event.
Short-term health insurance is available in most states (DC and 11 states do not have short-term plans available). It can serve as decent coverage if your other alternative is to remain uninsured. In most states, it’s the closest thing you can get to “real” health insurance if you find yourself needing to purchase a policy outside of open enrollment without a qualifying event.
For most of 2017 and 2018, short-term plans were capped at three months in duration, due to an Obama administration regulation. But HHS finalized new rules that drastically expanded the allowable duration of short-term plans as of October 2018.
The Obama administration’s HHS implemented the regulation to cap short-term plans at three months in an effort aimed at “curbing abuse” of short-term plans. At that point, under HHS Secretary Sylvia Matthews-Burwell, HHS noted that short-term plans are exempt from having to comply with ACA regulations specifically because they’re supposed to only be used to fill gaps in coverage — but instead, people had been using them for up to a year at a time, effectively removing healthy people from the ACA-compliant risk pool and destabilizing it over the long-run.
In 2017, several GOP Senators asked HHS to reverse this regulation and go back to allowing short-term plans to be issued for durations up to 364 days. And the Trump administration confirmed its commitment to rolling back the limitations on short-term plans in an October 2017 executive order. The new rules took effect in October 2018, implementing the following provisions:
- Short-term plans can now have initial terms of up to 364 days.
- Renewal of a short-term plan is allowed as long as the total duration of a single plan doesn’t exceed 36 months (people can string together multiple plans, from the same insurer or different insurers, and thus have short-term coverage for longer than 36 months, as long as they’re in a state that permits this).
- Short-term plan information must include a disclosure to help consumers understand the potential pitfalls of short-term plans and how they differ from individual health insurance.
The Biden administration may eventually impose new rules for short-term health plans, under the provisions of an executive order that President Biden signed in January 2021. That will be a somewhat lengthy process, however, as it would require proposed rules, a public comment period, and then a final rule (much the same as the process the Trump administration went through in 2018 to impose the relaxed rules that currently apply to short-term plans). This process had not yet begun as of early 2023. And it may not be entirely necessary for the time being, given the expansion of health insurance subsidies under the American Rescue Plan and Inflation Reduction Act (these subsidies can only be used for coverage purchased through the exchange, which makes short-term plans less attractive).
States can still impose stricter rules than the federal guidelines, and over half the states do so. Some are long-standing rules, while others are newly-adopted rules that states have implemented in an effort to prevent the Trump administration rules from destabilizing their individual insurance markets and pushing healthy people into less comprehensive coverage.
Although premium subsidies (a type of tax credit) are not available for short-term plans, the retail prices on these policies are more affordable than the retail price (ie, unsubsidized) on ACA-compliant plans, and they do still serve as a good stop-gap if you just need the policy to cover you for a few months when you’re in between other policies.
However, if your income makes you eligible for the Obamacare premium subsidies, it’s essential that you enroll through your state’s marketplace during open enrollment (or a special enrollment period triggered by a qualifying event like losing access to your employer-sponsored health insurance); otherwise, you’re missing out on comprehensive health insurance and a tax credit. And again, premium subsidies are currently larger and available to more people as a result of the American Rescue Plan.
Some short-term plans have provider networks, but others allow you to use any provider you choose (keep in mind, however, that you’ll likely be subject to balance billing if your plan doesn’t have a provider network, since the providers will not be bound by any contract with your insurer regarding the pricing for their services).
And short-term policies are not required to be renewable; the new federal ruleinsurers to offer renewable short-term plans, but does notthem to do so. Depending on your state’s regulations and your insurer’s business plan, you may be able to renew your short-term plans, or you may be able to purchase a new short-term policy when your existing one expires. But if you’re buying a new policy, the purchase will require new underwriting, and in most cases, the new policy will not cover pre-existing conditions, including any that began while you were covered under the first short-term policy.
Unlike ACA-compliant plans, short-term policies have benefit maximums. But the limits on some short-term plans tend to be more reasonable than the infamous pre-ACA “mini-med” plans that barely covered a few nights in the hospital. Lifetime maximums of $750,000 to $2 million are common on short-term plans. While this is not as good as regular individual insurance plans that no longer have annual or lifetime benefit caps, it’s roughly similar to a lot of the plans that were available pre-2014 in the individual market. And the concept of a “lifetime” limit doesn’t really matter when you’re talking about a plan that lasts for at most 36 months (the maximum amount of time a single plan can remain in effect under the new federal rules), since you won’t be able to purchase another short-term plan if you develop a serious health condition.
But you’ll see plenty of short-term policies with much lower benefit limits. As a general rule, you’ll want to focus on plans that offer at least $1 million in benefits — health care is shockingly expensive.
Short-term insurance applications
The application process is very simple for short-term policies. Once you select a plan, the online application is much shorter than it is for standard individual health insurance, and coverage can be effective as early as the next day.
There are no income-related questions (since short-term policies are not eligible for any of the ACA’s premium subsidies), and the medical history section is generally quite short – nowhere near as onerous as the pre-2014 individual health insurance applications were.
Keep in mind that although the medical history section generally only addresses the most serious conditions in order to determine whether or not the applicant is eligible for coverage, short-term plans generally have blanket disclaimers stating that no pre-existing conditions are covered.
And post-claims underwriting is common on short-term plans. So although the insurer may accept your application based simply on what you disclose when you apply, they can — and likely will — go back through your medical history with a fine-toothed comb if and when you have a significant claim. If they find anything indicating that the current claim might be related to a pre-existing condition, they can rescind your coverage or deny the claim. So although a short-term plan might work well to cover a broken leg, it’s going to be less useful if you end up with a health condition that tends to take a while to develop, as the insurer may determine that the condition, or something related to it, began before your coverage was in force. This story is a good example of how this works.
Clearly, short-term plans are not as good as the ACA-regulated policies that you can purchase during open enrollment or during a special enrollment period. Short-term insurance is not regulated by the ACA, so it doesn’t have to follow the ACA’s rules: The plans still have benefit maximums, and they are not required to cover the ten essential benefits. (Most often, short-term plans don’t cover maternity, prescription drugs, preventive care, or mental health/addiction treatment), they do not have to limit out-of-pocket maximums, and they do not cover pre-existing conditions. They also still use medical underwriting, so coverage is not guaranteed-issue.
The majority of short-term plans do not cover outpatient prescriptions. Using a pharmacy discount card may lower medication costs without health insurance, and some discount prices may be lower than an insurance copay.
Not a qualifying event: losing short-term coverage
Although loss of existing minimum essential coverage is a qualifying event that triggers a special open enrollment period for ACA-compliant individual market plans, short-term policies are not considered minimum essential coverage, so the loss of short-term coverage is not a qualifying event (loss of a short-term plana qualifying event for employer-sponsored coverage, however, so you’d be able to enroll in your employer’s plan when you short-term plan ends).
Let’s say you lose your job and your employer-sponsored health plan. You then have a 60-day window during which you can enroll in an ACA-compliant plan.
You also have the option to buy a short-term plan at that point, and it may be available with a term of up to a year, depending on where you live. But when the short-term plan ends, you would no longer have access to an ACA-compliant plan (you’d have to wait until the next open enrollment, and a plan selected during open enrollment would become effective on January 1) and although you could purchase another short-term plan, your eligibility would depend on your current medical history. Some short-term plan insurers offer guaranteed renewability under the new federal rules, meaning that people can renew the plan, without going through medical underwriting, and keep it for up to 36 months. But not all insurers offer this option.
Although short-term plans do not provide the level of coverage or consumer protections that the new ACA-compliant plans offer, obtaining a short-term policy is better than remaining uninsured. But your best bet is to maintain coverage under an ACA-compliant policy; if you’re not enrolled, you’ll want to do so if you experience a qualifying event (most people don’t take advantage of their qualifying events, perhaps unaware that their opportunity to enroll is limited).